Breast lipofilling
Breast lipofilling has become the procedure of choice for increasing breast volume and aesthetic enhancement.
Breast hypotrophy corresponds to insufficient volume in relation to the patient’s morphology. It either occurs immediately (since puberty) or appears later, following weight loss or pregnancy.
Presentation
Silicone gel implants (prostheses) are still the most common treatment for breast hypotrophy.
However, the technique of fat transfer, also known as lipofilling, has developed considerably since it was initially reserved for reconstructive surgery. Reconstructive surgery has made it possible to validate this technique and now offer our patients a safe and effective procedure.
In particular, modern lipofilling techniques do not present any particular diagnostic difficulties for a radiologist experienced in breast imaging.
Current scientific data shows no increase in the risk of developing a breast tumour after lipofilling. However, it is essential to carry out a pre-operative check-up (mammography and ultrasound) and then proceed according to the specialist radiologist’s recommendations.
Breast lipofilling is an increasingly popular technique because it uses natural, autologous material (the patient’s own fat). However, in some cases, breast implants will remain an option to be considered in consultation. It is also possible to combine the two techniques (composite augmentation).
Patients wishing to undergo a major breast augmentation may find the increase in volume from lipofilling insufficient. In this case, augmentation by prosthesis should be preferred, or it should be understood that a second lipofilling session may be necessary at a later date. This second session (carried out at least 6 months after the first operation) usually involves the same protocol and costs as the first step.
A lipofilling session generally increases the volume by one cup size. The ideal candidate is therefore someone who wants a moderate augmentation with a very natural appearance and no foreign prosthetic bodies. Of course, the patient must have an adequate supply of fat for the operation. But this is yet another advantage of lipofilling. This procedure helps to harmonise the figure by treating localised excess fat by liposuction (saddlebags, hips, abdomen, thighs, arms, etc.).
In cases of a genetic malformation or one resulting from trauma, partial assistance from the French Health Insurance may be requested. These include Poland syndrome, tuberous breasts and breast aplasia.
Procedure
Check-up before Breast Lipofilling
A pre-operative blood test and X-ray are carried out, as for all breast surgeries.
A consultation with my anaesthetist will be scheduled at least 48 hours before the breast lipofilling.
Aspirin and anti-inflammatory drugs should be avoided at all costs at least 8 days before the operation.
Smoking and breast lipofilling
Smoking can lead to significant scarring complications and infections.
Smoking can also cause cardiopulmonary complications during anaesthesia.
It is essential to stop smoking completely at least one month before and one month after the operation. The same applies to electronic cigarettes.
Anaesthesia and hospitalisation
A general anaesthetic is required for liposuction and fat transfer to the breasts. In most cases, breast lipofilling only requires outpatient hospitalisation (with discharge the same day).
The steps of breast lipofilling
Dr Olivier CLAUDE will make precise markings of the areas of fat to be removed and the recipient sites on the breast area.
The fat is removed with fine cannulas using a gentle liposuction technique. It is then centrifuged to ensure that only the best adipocytes are retained, in order to optimise the fat graft’s uptake. After this purification step, the fat is transferred to the breast using very fine cannulas through 1 to 2 mm incisions.
The operating time (from 1 hour to 4 hours) depends on the quantity of fat to be removed and the location of the donor areas.
Results
Post-operative care
Post-operative pain is generally moderate and mainly affects the donor areas. Bruising generally wanes rapidly, within 1 to 3 weeks. On the other hand, oedemas are eliminated more gradually, usually over a period of several weeks to several months.
Sun exposure and UV rays should be avoided for 2 months to prevent the risk of hyperpigmentation.
The result will gradually stabilise after the third month. Patients are generally very satisfied with the overall improvement in their figure. The breasts are rejuvenated, more attractive and more voluminous. In addition, the liposuction carried out for the removal of the fat increases the potential for improving well-being by harmonising the body’s shape (abdomen, hips, thighs, arms, etc.).
Most scientific studies estimate that on average 2/3 of the fat transferred will remain in the recipient site. And around 1/3 will be eliminated naturally by the body. The fat cells that remain alive in the breast will develop in the same way as other breast cells. They will therefore be sensitive to any weight loss or gain.
The risks
They are very rare, even though lipofilling is carried out using living tissue, which may present unpredictable reactions.
By choosing a surgeon qualified as a Specialist in Plastic and Aesthetic Surgery by the French Medical Council and graduate of a DESC (Diploma of Advanced Specialised Studies) in Plastic and Aesthetic Surgery, you limit these risks as much as possible.
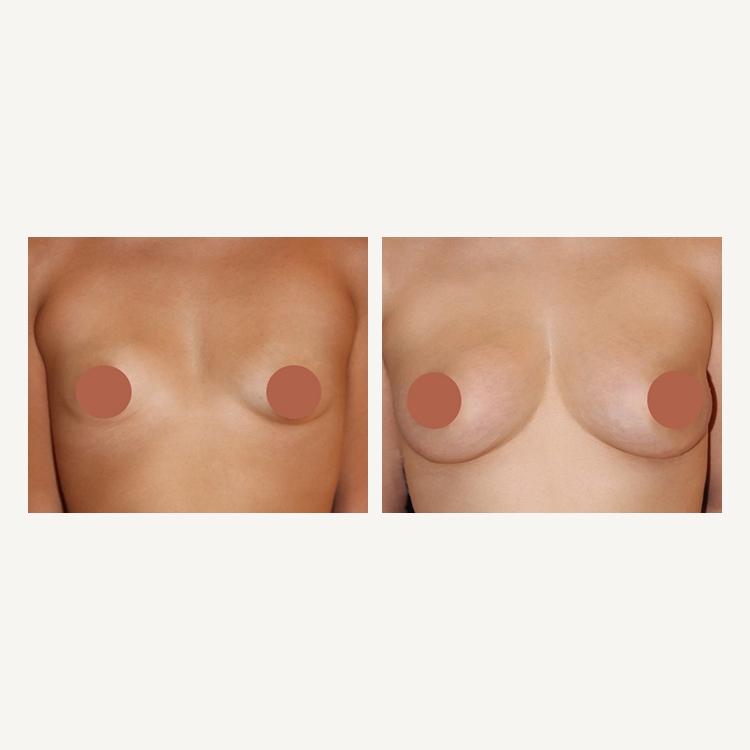
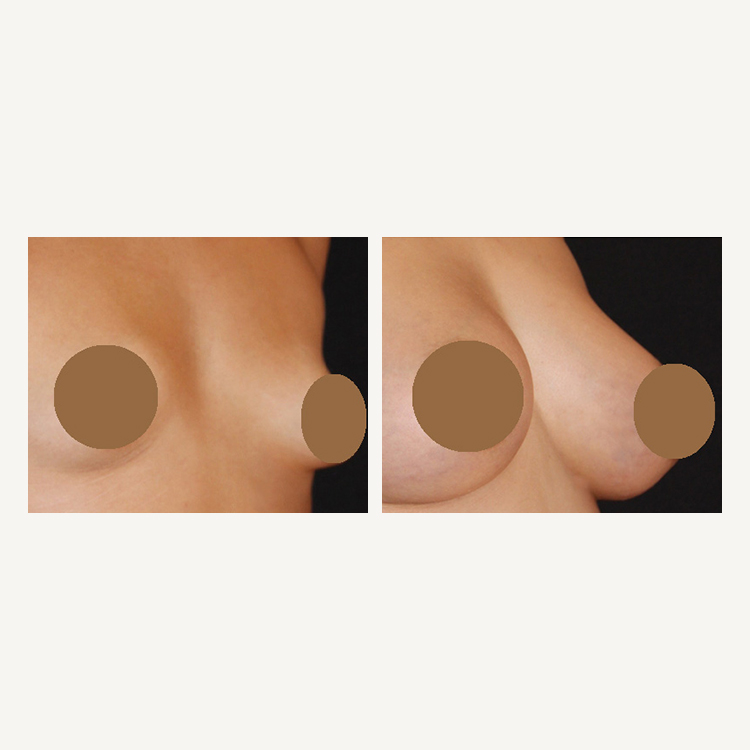
Before - After